Valsartan, amlodipine besilate.
Each film-coated tablet contains: Valsartan 160 mg/80 mg, amlodipine besilate equivalent to amlodipine 10 mg/5 mg.
Valsartan is a nonpeptide, orally active, and specific angiotensin II antagonist acting on the AT1 receptor subtype. Valsartan is a white to practically white fine powder, soluble in ethanol and methanol and slightly soluble in water. Valsartan's chemical name is N (1-oxopentyl)-N- [[2'-(1H-tetrazol-5-yl) [1,1'-biphenyl]-4-yl]methyl]-L-valine.
Its empirical formula is C24H29N5O3 and its molecular weight is 435.5.
Amlodipine besilate is the besilate salt of amlodipine, a dihydropyridine calcium channel blocker (CCB). It is a white to pale yellow crystalline powder, slightly soluble in water and sparingly soluble in ethanol. Amlodipine besilate's chemical name is 3 Ethyl-5-methyl(4RS)-2- [(2-aminoethoxy)methyl]-4-(2-chlorophenyl)-6-methyl-1,4 dihydropyridine-3,5-dicarboxylate benzenesulphonate.
Its empirical formula is C20H25ClN2O5.C6H6O3S and its molecular weight is 567.1.
Pharmacology: Pharmacodynamics: This fixed dose combination combines two antihypertensive compounds with complementary mechanisms to control blood pressure in patients with essential hypertension: Valsartan belongs to the angiotensin II antagonist class and amlodipine to the calcium antagonist class of medicines.
Valsartan: Valsartan is an orally active, potent and specific angiotensin II receptor antagonist. It acts selectively on the receptor subtype AT1, which is responsible for the known actions of angiotensin II. The increased plasma levels of angiotensin II following AT1 receptor blockade with valsartan may stimulate the unblocked receptor subtype AT2, which appears to counterbalance the effect of the AT1 receptor.
Valsartan does not exhibit any partial agonist activity at the AT1 receptor and has much (about 20,000 fold) greater affinity for the AT1 receptor than for the AT2 receptor. Valsartan does not inhibit ACE, also known as kininase II, which converts angiotensin I to angiotensin II and degrades bradykinin. Since there is no effect on ACE and no potentiation of bradykinin or substance P, angiotensin II antagonists are unlikely to be associated with coughing.
Administration of valsartan to patients with hypertension results in a drop in blood pressure without affecting pulse rate.
In most patients, after administration of a single oral dose, onset of antihypertensive activity occurs within 2 hours, and the peak drop in blood pressure is achieved within 4-6 hours. The antihypertensive effect persists over 24 hours after administration. During repeated administration, the maximum reduction in blood pressure with any dose is generally attained within 2-4 weeks and is sustained during long-term therapy. Abrupt withdrawal of valsartan has not been associated with rebound hypertension or other adverse clinical events.
Amlodipine: The amlodipine component of this fixed dose combination inhibits the transmembrane entry of calcium ions into cardiac and vascular smooth muscle. The mechanism of the antihypertensive action of amlodipine is due to a direct relaxant effect on vascular smooth muscle, causing reductions in peripheral vascular resistance and in blood pressure. Amlodipine binds to both dihydropyridine and non-dihydropyridine binding sites. The contractile processes of cardiac muscle and vascular smooth muscle are dependent upon the movement of extracellular calcium ions into these cells through specific ion channels.
Following administration of therapeutic doses to patients with hypertension, amlodipine produces vasodilation, resulting in a reduction of supine and standing blood pressures. These decreases in blood pressure are not accompanied by a significant change in heart rate or plasma catecholamine levels with chronic dosing.
Plasma concentrations correlate with effect in both young and elderly patients. In hypertensive patients with normal renal function, therapeutic doses of amlodipine resulted in a decrease in renal vascular resistance and an increase in glomerular filtration rate and effective renal plasma flow, without change in filtration fraction or proteinuria.
As with other calcium channel blockers, haemodynamic measurements of cardiac function at rest and during exercise (or pacing) in patients with normal ventricular function treated with amlodipine have generally demonstrated a small increase in cardiac index without significant influence on dP/dt or on left ventricular end diastolic pressure or volume. In haemodynamic studies, amlodipine has not been associated with a negative inotropic effect when administered in the therapeutic dose range to intact animals and humans, even when co-administered with beta blockers to humans.
Amlodipine does not change sinoatrial nodal function or atrioventricular conduction in intact animals or humans. In clinical studies in which amlodipine was administered in combination with beta blockers to patients with either hypertension or angina, no adverse effects on electrocardiographic parameters were observed.
Amlodipine/Valsartan: The combination of amlodipine and valsartan produces dose-related additive reduction in blood pressure across its therapeutic dose range. The antihypertensive effect of a single dose of the combination persisted for 24 hours.
Pharmacokinetics: Valsartan: Valsartan is rapidly absorbed following oral administration, with a bioavailability of about 23%. Peak plasma concentrations of valsartan occur 2 to 4 hours after an oral dose. It is between 94 and 97% bound to plasma proteins. Valsartan is not significantly metabolized and is excreted mainly via the bile as unchanged drug. The terminal elimination half-life is about 5 to 9 hours. Following an oral dose about 83% is excreted in the feces and 13% in urine.
Amlodipine: Amlodipine is well absorbed following oral administration with peak blood concentrations occurring after 6 to 12 hours. The bioavailability varies but is usually about 60 to 65%. Amlodipine is reported to be about 97.5% bound to plasma proteins. It has a prolonged terminal elimination half-life of 35 to 50 hours and steady-state plasma concentrations are not achieved until after 7 to 8 days of administration. Amlodipine is extensively metabolized in the liver; metabolites are mostly excreted in urine together with less than 10% of a dose as unchanged drug. Amlodipine is not removed by dialysis.
Treatment of essential hypertension.
It is indicated in patients whose blood pressure is not adequately controlled on valsartan or amlodipine monotherapy.
The recommended dose is one tablet per day.
Valsartan + Amlodipine may be administered in patients whose blood pressure is not adequately controlled with valsartan or amlodipine alone.
Individual dose titration with the components (i.e. amlodipine and valsartan) is recommended before changing to the fixed dose combination. When clinically appropriate, direct change from monotherapy to the fixed-dose combination may be considered.
For convenience, patients receiving valsartan and amlodipine from separate tablets/capsules may be switched to valsartan + amlodipine tablet containing the same component doses.
Renal impairment: No dosage adjustment is required for patients with mild to moderate renal impairment. Monitoring of potassium levels and creatinine is advised in moderate renal impairment.
Hepatic impairment: Caution should be exercised when administering to patients with hepatic impairment or biliary obstructive disorders. In patients with mild to moderate hepatic impairment without cholestasis, the maximum recommended dose is 80 mg valsartan.
Elderly (age 65 years or over): In elderly patients, caution is required when increasing the dosage.
Children and adolescents: Fixed dose combination of valsartan and amlodipine tablet is not recommended for use in patients aged below 18 years due to a lack of data on safety and efficacy.
Method of Administration: It can be used with or without food. It is recommended to be taken with some water.
Symptoms: There is no experience of overdose with valsartan/amlodipine tablet. The major symptom of overdose with valsartan is possibly pronounced hypotension with dizziness. Overdose with amlodipine may result in excessive peripheral vasodilation and, possibly, reflex tachycardia. Marked and potentially prolonged systemic hypotension up to and including shock with fatal outcome have been reported.
Treatment: If ingestion is recent, induction of vomiting or gastric lavage may be considered. Administration of activated charcoal to healthy volunteers immediately or up to two hours after ingestion of amlodipine has been shown to significantly decrease amlodipine absorption. Clinically significant hypotension due to valsartan/amlodipine tablet overdose calls for active cardiovascular support, including frequent monitoring of cardiac and respiratory function, elevation of extremities, and attention to circulating fluid volume and urine output. A vasoconstrictor may be helpful in restoring vascular tone and blood pressure, provided that there is no contraindication to its use. Intravenous calcium gluconate may be beneficial in reversing the effects of calcium channel blockade. Both valsartan and amlodipine are unlikely to be removed by haemodialysis.
Hypersensitivity to the active substances, to dihydropyridine derivatives, or to any of the excipients.
Severe hepatic impairment, biliary cirrhosis or cholestasis.
Severe renal impairment (GFR<30 mL/min/1.73 m2) and patients undergoing dialysis.
Second and third trimesters of pregnancy.
Sodium- and/or volume-depleted patients: In patients with an activated renin-angiotensin system (such as volume- and/or salt depleted patients receiving high doses of diuretics) who are receiving angiotensin receptor blockers, symptomatic hypotension may occur. Correction of this condition prior to administration or close medical supervision at the start of treatment is recommended. If hypotension occurs with fixed dose combination of valsartan and amlodipine tablet, the patient should be placed in the supine position and, if necessary, given an intravenous infusion of normal saline. Treatment can be continued once blood pressure has been stabilized.
Hyperkalaemia: Concomitant use with potassium supplements, potassium-sparing diuretics, salt substitutes containing potassium, or other medicinal products that may increase potassium levels (heparin, etc.) should be undertaken with caution and with frequent monitoring of potassium levels.
Renal artery stenosis: No data are available in patients with bilateral renal artery stenosis or stenosis to a solitary kidney.
Kidney transplantation: To date there is no experience of the safe use in patients who have had a recent kidney transplantation.
Hepatic impairment: Valsartan is mostly eliminated unchanged via the bile, whereas amlodipine is extensively metabolised by the liver. Particular caution should be exercised when administering it to patients with mild to moderate hepatic impairment or biliary obstructive disorders.
In patients with mild to moderate hepatic impairment without cholestasis, the maximum recommended dose is 80 mg valsartan.
Renal impairment: No dosage adjustment is required for patients with mild to moderate renal impairment (GFR>30 ml/min/1.73 m2). Monitoring of potassium levels and creatinine is advised in moderate renal impairment.
Primary hyperaldosteronism: Patients with primary hyperaldosteronism should not be treated with the angiotensin II antagonist valsartan as their renin-angiotensin system is affected by the primary disease.
Heart failure: As a consequence of the inhibition of the renin-angiotensin-aldosterone system, changes in renal function may be anticipated in susceptible individuals. In patients with severe heart failure whose renal function may depend on the activity of the renin angiotensin-aldosterone system, treatment with angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor antagonists has been associated with oliguria and/or progressive azotaemia and (rarely) with acute renal failure and/or death. Similar outcomes have been reported with valsartan.
Aortic and mitral valve stenosis, obstructive hypertrophic cardiomyopathy: As with all other vasodilators, special caution is indicated in patients suffering from aortic or mitral stenosis, or obstructive hypertrophic cardiomyopathy.
Use in pregnancy: Angiotensin II Receptor Antagonists (AIIRAs) should not be initiated during pregnancy. Unless continued AIIRA therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with AIIRAs should be stopped immediately, and, if appropriate, alternative therapy should be started.
The use of Angiotensin II Receptor Antagonists (AIIRAs) is not recommended during the first trimester of pregnancy. The use of AIIRAs is contraindicated during the second and third trimesters of pregnancy.
Epidemiological evidence regarding the risk of teratogenicity following exposure to ACE inhibitors during the first trimester of pregnancy has not been conclusive; however a small increase in risk cannot be excluded. Whilst there is no controlled epidemiological data on the risk with Angiotensin II Receptor Antagonists (AIIRAs), similar risks may exist for this class of drugs. Unless continued AIIRA therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy.
When pregnancy is diagnosed, treatment with AIIRAs should be stopped immediately, and, if appropriate, alternative therapy should be started.
Exposure to AIIRA therapy during the second and third trimesters is known to induce human foetotoxicity (decreased renal function, oligohydramnios, skull ossification retardation) and neonatal toxicity (renal failure, hypotension, hyperkalaemia).
Should exposure to AIIRAs have occurred from the second trimester of pregnancy, ultrasound check of renal function and skull is recommended.
Infants whose mothers have taken AIIRAs should be closely observed for hypotension.
Use in Lactation: It is not recommended and alternative treatments with better established safety profiles during breast-feeding are preferable, especially while nursing a newborn or preterm infant.
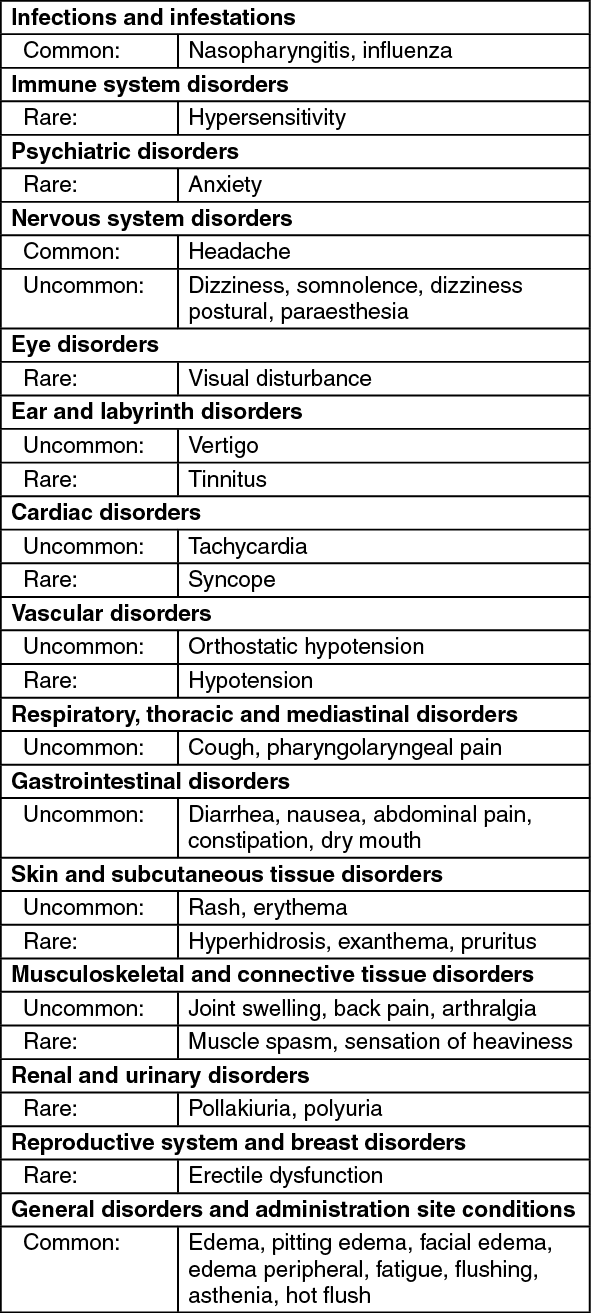
Adverse reactions have been ranked under headings of frequency using the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000, including isolated reports). (See table.)
 Click on icon to see table/diagram/image
Additional information on the combination:
Click on icon to see table/diagram/image
Additional information on the combination: Peripheral edema, a recognized adverse effect of amlodipine, was generally observed at a lower incidence in patients who received the amlodipine/valsartan combination than in those who received amlodipine alone.
Additional information on the individual components: Valsartan: Not known: Decrease in haemoglobin, decrease in haematocrit, neutropenia, thrombocytopenia, increase of serum potassium, elevation of liver function values including increase of serum bilirubin, renal failure and impairment, elevation of serum creatinine, angioedema, myalgia, vasculitis, hypersensitivity including serum sickness.
Amlodipine: Common: Vomiting.
Uncommon: Alopecia, altered bowel habits, dyspepsia, dyspnoea, rhinitis, gastritis, gingival hyperplasia, gynaecomastia, hyperglycaemia, impotence, increased urinary frequency, leucopenia, malaise, mood changes, myalgia, peripheral neuropathy, pancreatitis, hepatitis, thrombocytopenia, vasculitis, angioedema and erythema multiforme.
Rare: Arrhythmia, myocardial infarction. Rarely, patients, particularly those with severe obstructive coronary artery disease, have developed increased frequency, duration or severity of angina or acute myocardial infarction on starting calcium channel blocker therapy or at the time of dosage increase. Arrhythmia (including ventricular tachycardia and atrial fibrillation) has also been reported. These adverse events may not be distinguishable from the natural history of the underlying disease.
Very rare: Cholestatic jaundice, AST and ALT increase, purpura, rash and pruritus. Exceptional cases of extrapyramidal syndrome have been reported.
Interactions linked to valsartan.
Concomitant use not recommended.
Lithium: Reversible increases in serum lithium concentrations and toxicity have been reported in literature during concurrent use of ACE inhibitors. Despite the lack of experience with concomitant use of valsartan and lithium, this combination is not recommended. If the combination proves necessary, careful monitoring of serum lithium levels is recommended.
Potassium-sparing diuretics, potassium supplements, salt substitutes containing potassium and other substances that may increase potassium levels: If a medicinal product that affects potassium levels is to be prescribed in combination with valsartan, monitoring of potassium plasma levels is advised.
Caution required with concomitant use: Non-steroidal anti-inflammatory drugs (NSAIDs), including selective COX-2 inhibitors, acetylsalicylic acid (>3 g/day), and non-selective NSAIDs.
When angiotensin II antagonists are administered simultaneously with NSAIDs, attenuation of the antihypertensive effect may occur. Furthermore, concomitant use of angiotensin II antagonists and NSAIDs may lead to an increased risk of worsening of renal function and an increase in serum potassium. Therefore, monitoring of renal function at the beginning of the treatment is recommended, as well as adequate hydration of the patient.
Others: In monotherapy with valsartan, no interactions of clinical significance have been found with the following substances: cimetidine, warfarin, furosemide, digoxin, atenolol, indometacin, hydrochlorothiazide, amlodipine, glibenclamide.
To be taken into account with concomitant use: Other antihypertensive agents: Commonly used antihypertensive agents (e.g. alpha blockers, diuretics) and other medicinal products which may cause hypotensive adverse effects (e.g. tricyclic antidepressants, alpha blockers for treatment of benign prostate hyperplasia) may increase the antihypertensive effect of the combination.
Interactions linked to amlodipine: Caution required with concomitant use: CYP3A4 inhibitors: Diltiazem inhibits the metabolism of amlodipine, probably via CYP3A4 (plasma concentration increases by approximately 50% and the effect of amlodipine is increased). The possibility that more potent inhibitors of CYP3A4 (i.e. ketoconazole, itraconazole, ritonavir) may increase the plasma concentration of amlodipine to a greater extent than diltiazem cannot be excluded.
CYP3A4 inducers (anticonvulsant agents [e.g. carbamazepine, phenobarbital, phenytoin, fosphenytoin, primidone], rifampicin, Hypericum perforatum [St. John's Wort]).
Co-administration may lead to reduced plasma concentrations of amlodipine. Clinical monitoring is indicated, with possible dosage adjustment of amlodipine during the treatment with the inducer and after its withdrawal.
To be taken into account with concomitant use: Others: In monotherapy, amlodipine has been safely administered with thiazide diuretics, beta blockers, ACE inhibitors, long-acting nitrates, sublingual nitroglycerin, digoxin, warfarin, atorvastatin, sildenafil, antacid medicines (aluminum hydroxide gel, magnesium hydroxide, simeticone), cimetidine, non-steroidal anti-inflammatory drugs, antibiotics and oral hypoglycemic drugs.
Store at temperatures not exceeding 30°C.
C09DB01 - valsartan and amlodipine ; Belongs to the class of angiotensin II receptor blockers (ARBs) and calcium channel blockers. Used in the treatment of cardiovascular disease.
Amloval 160/10 FC tab
30's (P1,285.5/box)
Amloval 160/5 FC tab
30's (P990/box)
Amloval 80/5 FC tab
30's (P1,285.5/box)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
